
November 12, 2012
“What we wanted to do was assess the prevalence of AAA at initial CTC screening, and then track what happens to patients over five years, and we also wanted to assess the incidence of new aneurysms that popped up after an initial screening CTC,” said Dr. Dustin Pooler, currently a surgical resident at the University of Wisconsin, in an interview with AuntMinnie.com.
Many individuals at risk for colorectal polyps are also at risk for AAA. The U.S. Preventive Services Task Force (USPSTF) recommends one-time screening by ultrasound for men ages 65 to 75 years who have ever smoked.
In the U.K., the National Health Service is a bit more proactive, recommending AAA screening of all men at age 65, based on the 10-year Multicentre Aneurysm Screening Study (MASS) showing that only 192 at-risk patients need to be screened to prevent one death from AAA over 10 years (Lancet, November 16, 2002, Vol. 360:9345, pp. 1531-1539).
The cross-sectional nature of CTC allows for the detection of extracolonic abnormalities, and there is significant overlap in the population recommended for CTC and the population recommended for AAA screening. Most important, AAA screening could be performed at CTC without additional cost or radiation exposure — potentially making CTC more cost-effective, researchers said in a presentation at the American Roentgen Ray Society (ARRS) meeting in May in San Diego.
In their study, Pooler and colleagues Dr. David Kim and Dr. Perry Pickhardt examined 1,061 consecutive asymptomatic adults (501 men, 560 women; mean age, 57.2 ± 7.6 years) who underwent first-time screening virtual colonoscopy over a 13-month period. Researchers recorded AAA detected in the index exam as part of a routine search for extracolonic findings.
Forty-two patients were lost to follow-up, leaving 1,019 to be followed longitudinally for a mean 4.81 years via review of electronic medical records, Pooler said. Known aneurysms were followed for growth, and new ones were recorded.
“We basically followed them with a medical record review, going through their visits with doctors and hospitalizations,” Pooler told AuntMinnie.com. “We only had imaging in 267, and there were no reports of anyone going to the hospital for an aneurysm that ruptured or something like that.”
At index CTC, AAA was detected in 0.8% of the patients (9/1,061; 95% confidence interval: 0.4%-1.6%), with a mean diameter of 3.10 ± 0.2 cm. Additional abdominal vascular aneurysms (n = 5) included common iliac artery (n = 3), femoral artery (n = 1), and splenic arteries (n = 1), for an overall prevalence of 1.3% (14/1,061).
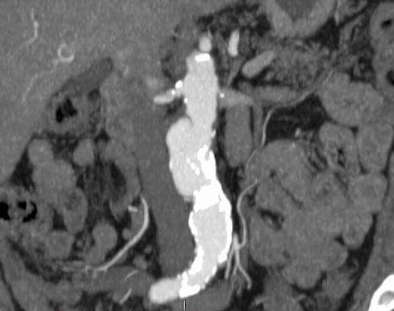 |
| Abdominal aortic aneurysm detected at CTC screening. Image courtesy of Dr. Dustin Pooler. |
None of the 267 people who had follow-up abdominal CT exams had aneurysms detected, and because this was a clinically based study, not all patients were followed up with a second imaging exam during the study interval, Pooler said.
However, of those who did undergo additional imaging, no patients ended up developing a new triple AAA. Finally, the medical record review showed no new aneurysms forming among the remaining patients.
“This makes sense because CT is quite accurate for the detection of AAA, and AAA tends to be something that develops a little bit more slowly over time,” he said. “So it would make sense that if you didn’t have AAA two to three years ago, your chances of having one three years four years later is rare.”
Over 4.81 years, known aneurysms increased by an average 0.6 cm to 3.80 cm in diameter. One patient with an aneurysm detected at the initial CTC screening underwent endovascular repair with no complications.
“This was someone who went on to benefit,” Pooler said. “Of the other patients, none had gone to surgery and they went into imaging follow-up based on CT, so their aneurysm was detected and they were able to get appropriate follow-up.”
Study limitations included potential sample bias, inasmuch as screening was dependent on referral by a primary physician. Also, there were a limited number of patients who were negative at the initial screening who had an imaging study during the follow-up interval.
Overall, the study found AAA in more than 1% of screening CTC patients, mostly men, and they showed a mean growth of about 0.5 cm during the follow-up period. There were no incident aneurysms in patients who were negative at the initial CTC screening.
Extracolonic benefit
The results suggest an extracolonic benefit to CTC screening with no additional cost or radiation exposure, and that there could be a screening role in using CTC to look for abdominal aortic aneurysms, he said.
“There’s already evidence to show there’s a benefit to doing a one-time AAA screening in a patient population that overlaps pretty well with a patient population that should be getting screened for colon cancer,” Pooler said. “So in terms of a cost-saving measure, and based on the fact that CT is quite good at detecting AAA, we don’t see any reason why VC wouldn’t be able to serve that role and why you shouldn’t be able to screen for AAA.”
If it works, why not throw in the kitchen sink, and maximize CTC’s cost-effectiveness by including AAA and osteoporosis studies based on CTC data for every individual referred for colorectal cancer screening?
“Each test would need to be assessed and research would need to be done to determine if it’s beneficial to the patient and cost-effective before they would be included,” he said.
“We already know there’s not any benefit to the full-body scan — that hasn’t really panned out,” Pooler said. “And we don’t want to treat VC as a whole-body scan; we would like it to be targeted. That’s what we’ve targeted in research: how can it be effective and how can it not be effective.”